A Comprehensive Review of Low-Speed Rear Impact Volunteer Studies and a Comparison to Real-World Outcomes
posted: Oct. 25, 2019.
Whiplash-associated disorder (WAD) is a major concern worldwide with neck pain being the most common complaint following a motor vehicle collision.1 The cost of whiplash is difficult to quantify, due to variations in definitions and data collection, but in the United States, WAD has been estimated to cost $2.7 billion per year. The United Kingdom, with an annual cost of over $3 billion, has been called “the whiplash capital of the world.”2,3 The UK also reports that about 70% of motor vehicle collision personal injury claims are for WAD.4
WAD has been studied using a variety of data sources and methods to answer specific or general questions about its etiology. These studies include retrospective analyses of the association between occupant characteristics, symptoms, and crash parameters as well as prospective testing using crash test dummies, cadavers, and human volunteers. Retrospective studies have found that crash environment, subject's age, anticipation of the crash, and gender play a role in the duration and severity of reported symptoms, revealing a mix of biological, psychological, and social factors involved in post-crash outcomes (63). Castro12 published a study documenting WAD symptoms in patients following a placebo rear-end collision. Twenty percent of these subjects reported whiplash-like symptoms within 3 days of the event, even though no crash took place [13]. Thus, a confounding factor in assessing WAD is that researchers use symptoms synonymously with injury. Pain is expected to immediately follow an acute traumatic injury, but the expression of pain does not necessarily mean that there has been an acute traumatic injury.
From a biomechanical perspective, low-speed events have been evaluated extensively using human volunteers.5–68 Experiments using large numbers of volunteers exposed to rear impacts have produced data regarding the kinematic and kinetic responses and reported symptoms of human occupants. These studies have used a wide range of subjects and conditions such as impact severity, awareness of the impending impact, initial position, posture, and seat and head restraint characteristics. The results reported vary by study and include head acceleration, kinematics, and high-speed cineradiography of the cervical spine during the test.
Previous authors have studied the volunteer literature at various times. In 1996, Szabo and Welcher58 compiled 284 volunteer crash tests at changes in velocity (delta V) up to 14 kph, including 10 publications and three sources of unpublished data. None of the volunteers had symptoms lasting longer than 7 days. In 2005, Moss et al.69 analyzed 28 studies, representing 206 exposures. Fifty-nine percent of those exposed had symptoms, most of which resolved within 12 days. In 2007, Nordhoff et al.70 published a collection of 18 papers and 62 abstracts regarding rear-end collisions, which represented a review of the state of biomechanical literature at that time. There has been extensive volunteer testing since, but no subsequent review until now.
The goal of this paper is to add to the number of volunteer exposures available for analysis and compare these data with real-world collisions of similar severity from the NASS CDS database.
MATERIALS AND METHODS
For this study, symptoms are not synonymous with injury, but only indicate that the volunteer reported symptoms for a given period of time. Within volunteer studies, symptoms are not only likely related to muscle strain but also may be due to the psychological influence of these events71 and, therefore, are not necessarily indicative of structural tissue damage. In this study, injury is defined as traumatic structural damage to a tissue (bone, ligament, tendon, disc) with an objective finding. If no injury is described in the article, then that volunteer is denoted as uninjured in our dataset. This is a reasonable assumption, as ethically authors would be obligated to report any traumatic injury and, from a scientific standpoint any objective injury would be described to provide data regarding what injuries are produced and under what conditions. Strains should also be differentiated from sprains in that strains are injuries of the musculature caused by stretching and tearing of the muscle fibers, whereas sprains are injuries of the ligaments resulting from stretching or tearing of the ligamentous tissue.
Data Sources
Volunteer Studies
The data used for this study were collected from individually published studies that performed rear impact testing on human volunteers. Studies were identified through an exhaustive search of the literature as well as obtaining referenced work within the articles themselves. Articles from the same authors or institution were screened to identify publications reporting the same tests to ensure that a single volunteer exposure was not included multiple times. When reported, volunteer or test identification was recorded in the final dataset to facilitate identification of repeated reporting of the same exposure. Some studies were excluded due to lack of sufficient data to identify the number of volunteers or number of exposures experienced by the volunteers. Otherwise, all studies using human volunteers were included regardless of the level of information provided regarding the test conditions.
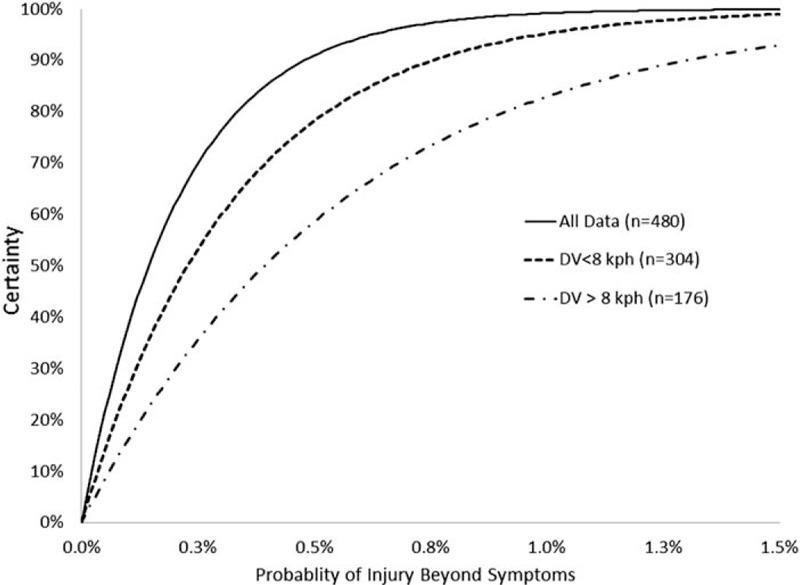
Operating-characteristic (OC) curves were created to assess the utility of the volunteer dataset in making predictions regarding the overall population. OC curves are commonly used to assess the statistical power (Pa) that a sample (n) has in predicting the likelihood that there were no defective items (seriously injured volunteers) in the population of human subjects involved in experimental rear impacts. For this study, OC curves were calculated to determine the level of statistical confidence that the human population will not sustain an injury beyond the reported short-term symptoms during a minor rear impact based on the number of available individual volunteers. Multiple exposures of a single volunteer were not included in the OC curve calculations. The probability of acceptance is determined by the binomial distribution and assumes that the population is a random process taken from an infinite lot. The probability of acceptance is the likelihood that the actual number of defectives (d) is less than or equal to the acceptable number (c). 
In this study, the OC curve provides the level of certainty for an assumed underlying risk of injury for the population based on the number of injuries within the sample of volunteers. The OC curve will provide the likelihood that no volunteer would sustain an injury for a given number of samples and an assumed level of risk. The higher the underlying risk of injury, the more likely that an injured volunteer would be within the sample.
Real-World Outcomes
A second dataset of rear impacts was analyzed using the National Automotive Sample System (NASS) Crashworthiness Data System (CDS) database. The NASS database represents a collection of real-world crashes that are investigated by the National Highway Traffic Safety Administration (NHTSA). Approximately 4000 to 5000 crashes are investigated annually and about half are reconstructed to determine the change in speed experienced by the struck vehicle. In addition, a large number of variables describing the accident, vehicle, and occupants involved are collected. The NASS database was queried for vehicles exposed to rear impacts defined as having a Principal Direction of Force (PDOF) between 5 and 7 o’clock. Only those exposed to a single event, meaning the vehicle did not contact any other object during the accident, were included. The occupants were limited to the front outboard positions over the age of 16. Only vehicles with a known change in speed and occupants with a known treatment were included to ensure proper documentation of injured and uninjured occupants. The NASS database contains information regarding the injuries sustained by the occupants in the form of their Abbreviated Injury Scale (AIS) identifier.72 This number identifies the type of injury and the specific anatomical structure involved. The NASS dataset uses a specific code, which is defined as whiplash or a neck muscle strain (640278). This AIS code was used to identify occupants diagnosed with neck strain or who self-reported the presence of neck strain. The occurrence of neck strain in the NASS database was compared with that within the volunteer dataset
The two refined datasets were analyzed using the Statistical Analysis Software (SAS, 9.4, Cary, NC) and Microsoft Excel (2013, Redmond, WA). Statistics were performed to provide an understanding of the overall make-up of the available testing using human volunteers. Additional analyses were performed to answer specific questions based on the data available. Differences among proportional outcomes were tested for significance using the Fisher exact test.
RESULTS
Volunteer Database
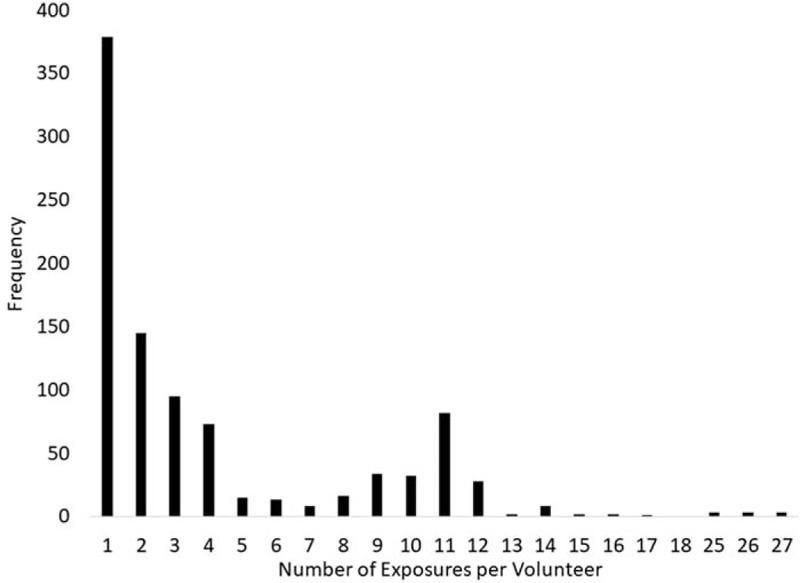
A complete collection of the available volunteer literature resulted in a dataset of 1984 total volunteer exposures from 51 individual studies.5–10,12,15–18,22–26,28–32,34–41,43,46–54,56–59,61–64,66–68,73 On average, each study performed 40 tests with a range from 1 to 484 tests and used 51 subjects with a range of 1 to 65 volunteers per study. Many of the volunteers experienced more than one exposure (Figure 1). Within the complete dataset, 52% of the impacts were at a delta-V less than 2 mph and a significant number had repeated exposures at very low (<1.5 kph, ∼1 g impacts) severities. The acceleration produced by these impacts is not expected to produce a meaningful response of the volunteers in terms of producing injury and the large number of these exposures would weigh the dataset toward more minor events. Therefore, impacts with a change in speed less than 1.5 kph were removed from the complete dataset. This reduced the dataset to a total of 1251 volunteer exposures (Figure 2) and contained volunteers who were exposed to multiple impacts at the same or increasing severity.
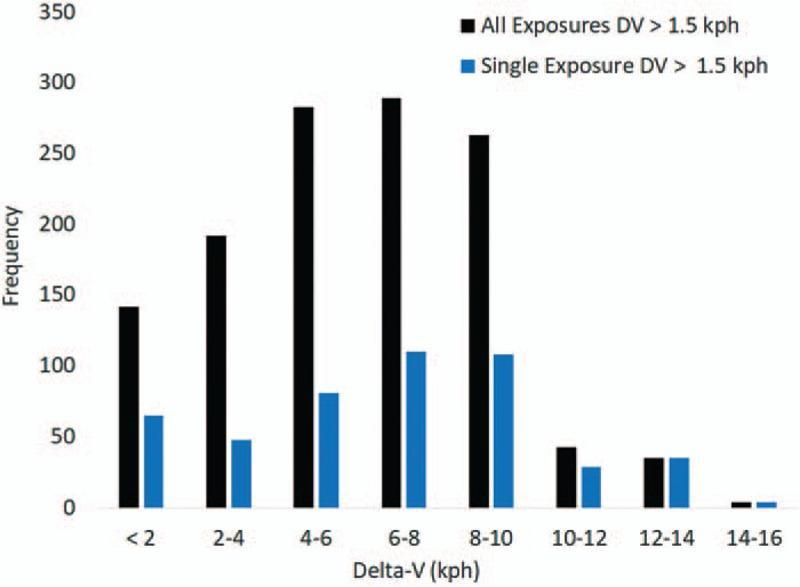
As the outcome of multiple impacts on a single volunteer would weigh the data artificially, separate analyses were conducted on a dataset containing repeated testing and a second dataset that only contained a single impact exposure with the greatest change in velocity. Eliminating the multiple impacts produced a dataset with 480 volunteers with a single exposure (Figure 2). In this dataset with a single exposure, if the volunteer reported symptoms following their exposure then the observation was counted as causing the symptom. In the dataset with multiple exposures for a single volunteer, if the volunteer reported symptoms after exposure to the entire series, each exposure was counted as causing symptoms unless the study was designed with a time gap between testing to allow symptoms to subside.
Symptoms
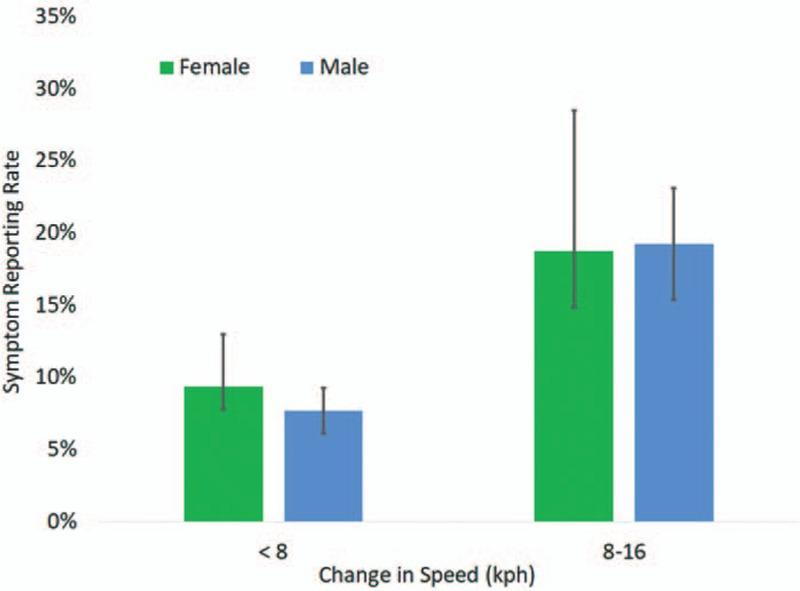
The incidence of neck symptoms within the volunteer database was assessed as a function of impact severity within the dataset containing single exposures above a delta-V of 1.5 kph. The symptom rate for males and females were similar and increased as delta-V increased from less than 8 to greater than 8 kph (Figure 3). On the basis of Fisher exact tests, only males (P = 0.026) showed a statistically significant increase in symptom rate between the 1.5 to 8 kph and 8 to 16 kph groups. There was no difference between symptom rates for the male and female volunteers. The lack of difference by gender means the entire dataset can be analyzed without accounting for gender.
Within the single exposure data, the majority of the volunteers were unaware of the impending impact (n = 422). A smaller portion indicated that the volunteer was braced (n = 28) at the time of the rear impact. The proportion of volunteers reporting symptoms was greater for those who were braced (25%) than those who were not braced (7.6%). This difference was statistically significant using Fisher exact test (P = 0.0065). The difference between impact severity for the braced (7.2, Std. Dev = 2.3 kph) and relaxed (6.3, Std. Dev = 3.3 kph) volunteers was 1 kph and was not statistically significant (P = 0.51).
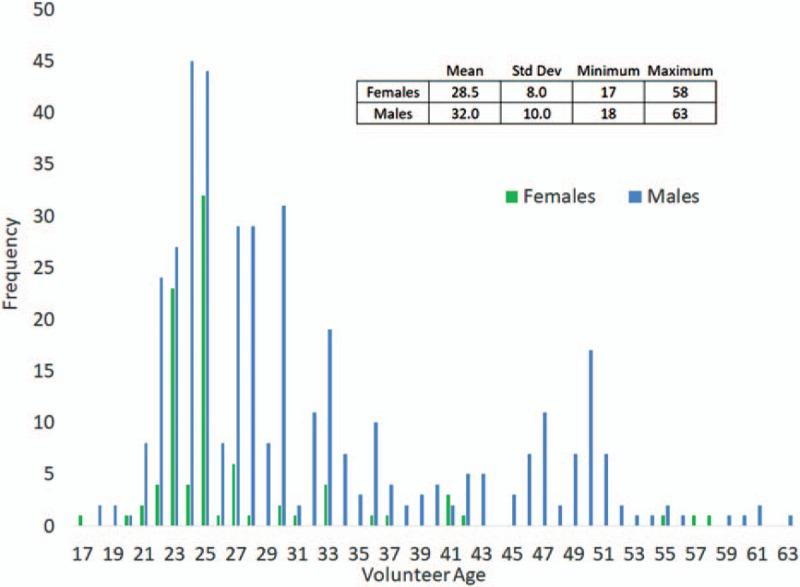
Volunteer age was similar between males and females and ranged from 17 to 63 years (Figure 4). Within the single exposure data, volunteers who reported symptoms tended to be older (age = 37) than those who did not have symptoms (age = 31) (P < 0.0001).
Operating Characteristic Curve
The OC curve was calculated on the basis of the 480 nonrepeated tests within the volunteer dataset. The level of certainty based on the entire single exposure dataset (Figure 5) showed that there would be a 95% chance of having a volunteer within the dataset that did sustain an injury if the underlying risk of injury was about 0.6%. For impacts with a change in speed less than and greater than 8 kph, the certainty was 84% and 64%, respectively. Therefore, the large number of single exposure volunteer tests provide a strong indicator that the likelihood of injury during a minor rear impact is remote. This is consistent with the general acceptance that human volunteers can be exposed to these events without a risk of injury.
Head and Neck Biomechanics
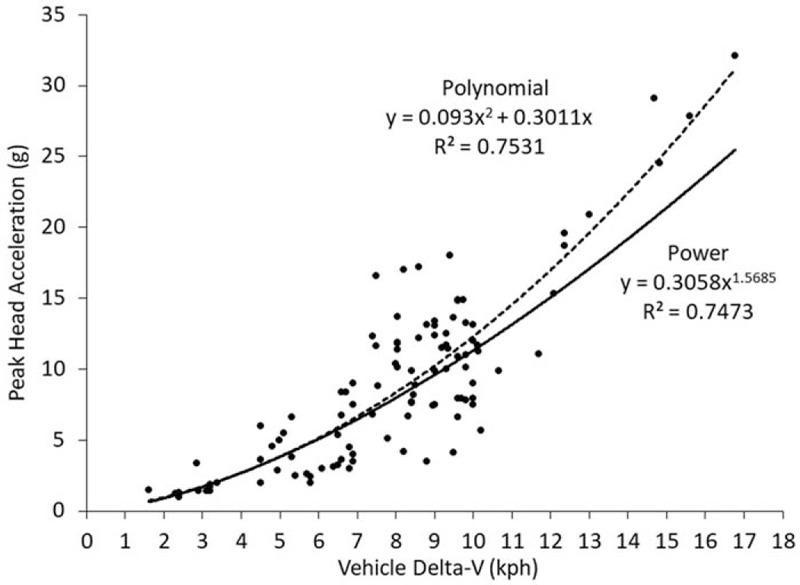
The head acceleration and neck moments reported within the volunteer studies were summarized. Twelve studies reported head acceleration experienced by the volunteers.5,15,23,26,30,32,37,38,40,59,67,68 These studies provide 125 data points for head acceleration as a function of vehicle change in speed (Figure 6). These points were fit to a polynomial and power trendline, which produced similar accuracy. For the average change in speed of 7.2 kph (Std. Dev. = 3.2 kph), the average head acceleration was 8 g (Std. Dev. = 6 g).
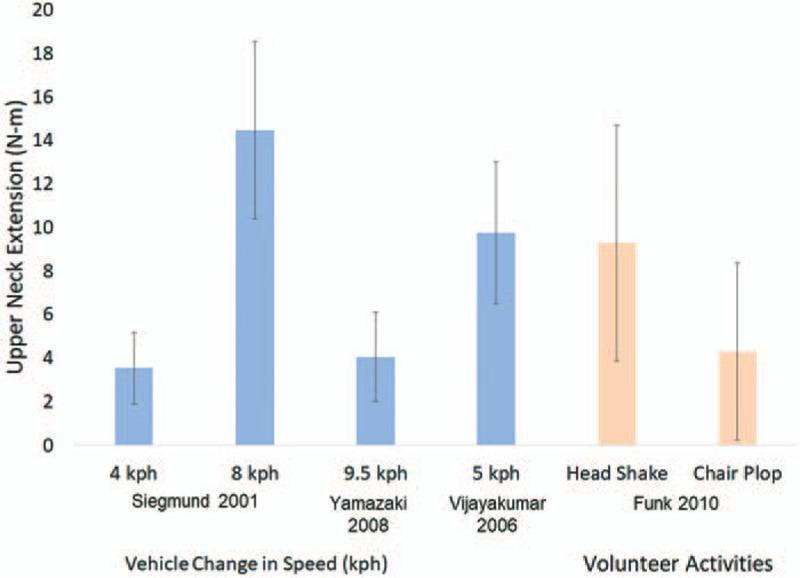
Neck moments experienced by human volunteers have also been reported within previous studies (Figure 7). The values for neck extension were reported for volunteers with and without head restraints.64,74,75 These studies demonstrate the primary loading condition for the cervical spine in rear impacts is comprised of tension and extension forces. The magnitude of the extension moment experienced by the human volunteers during rear impacts is similar to those experienced by volunteer during everyday and vigorous activities.64,76,77
Real-world Rear Impacts
The dataset of real-world crashes derived from the NASS database consisted of 2058 raw occupants that represent 1,313,136 occupants nationally. Within these occupants, 644 raw and 515,601 weighted occupants were exposed to a rear impact with a change in speed of 16 kph or less. The average age of the complete set of occupants was 38 years and the average change in speed, or delta-V was 20 kph.
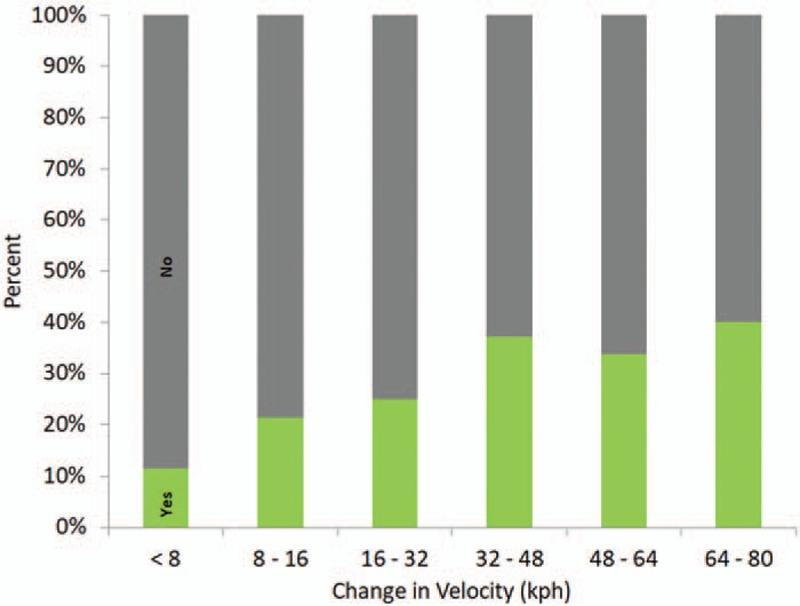
The distribution of neck strain within the real-world rear impacts was evaluated using the AIS code within NASS. The distribution of neck strain demonstrated a slight dependence on change in speed, but only across large changes of impact severity (Figure 8). For impacts with a change in speed less than 16 kph, the rate of neck strain was 21%.
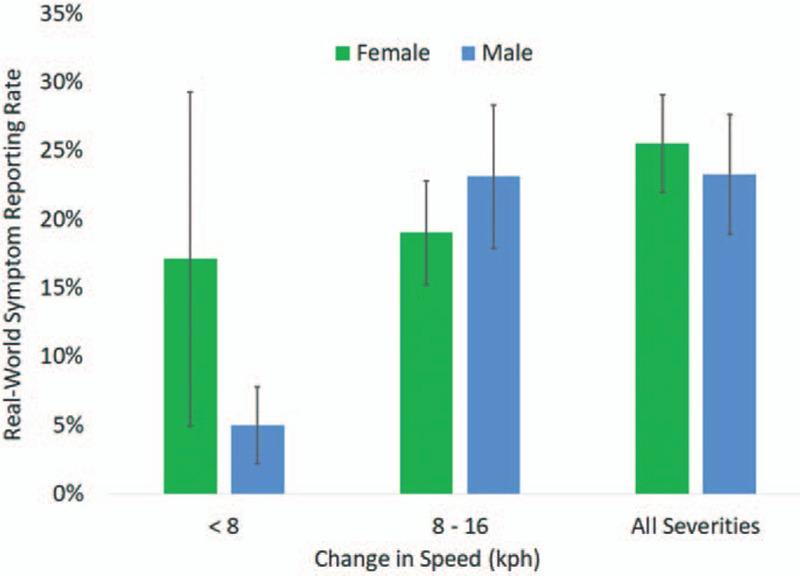
Within real-world rear impacts with a change in speed below 8 kph, females had a higher rate of symptoms; however, this difference was not statistically significant (P = 0.39). For impacts with a change in speed between 8 and 16 kph, the incidence of neck strain was greater for males, with no statistically significance from females (P = 0.60) (Figure 9). The rate of neck strain for rear impacts with a change in speed between 0 and 16 kph was 19% and 22% for the females and males, respectively.
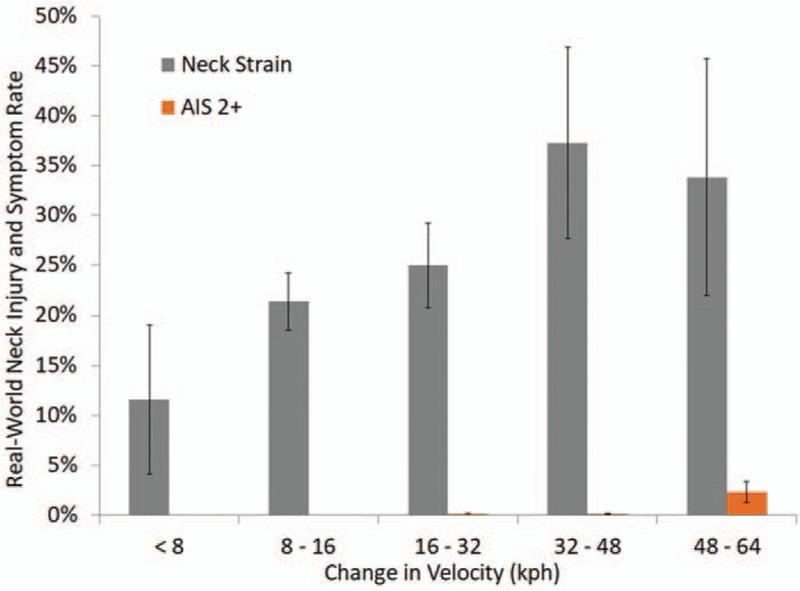
Overall, the real-world data showed that the risk of any neck injury (AIS 2+) beyond muscle strain is small, even for high levels of change in speed (Figure 10). The likelihood of neck strain was significantly greater than more consequential, AIS 2+ injuries.
Injury risk was also assessed using logistic regression analyses. For neck strain and AIS 2+ injuries, only a change in speed was found to be statistically significant. Age, gender, belt use, head restraint, and vehicle type were not statistically significant in predicting neck strain or AIS 2+ neck injuries.
DISCUSSION
The results of this study, using both experiment-based and real-world data, reinforce the general acceptance that human volunteers can be safely exposed to rear impacts of less than 18 kph without a meaningful risk of injury. Interestingly, both data sources produced similar rates of neck strain by gender and impact severity. This indicates that there is no reporting bias by the volunteers, some of whom are the authors of the articles. In addition, the similarity between the volunteer and real-world data indicate that any minor variation in head or body position that may be present in real-world collisions did not result in an increased rate of injury. Contrary to common belief, the volunteers that were reported as being braced had a higher rate of reporting symptoms than those that were not. The small underlying risk of injury indicated by the operating characteristic curve for the volunteer studies is consistent with the small risk of neck injury predicted by the real-world analysis.
The lack of injury to the volunteers results from the minor nature of the motion and forces they are exposed to as well as the direction of the forces applied to their bodies. Biomechanical research has shown that in order to produce a specific injury, a specific set of forces are required at the proper location and orientation. Experimental studies of the cervical and lumbar spine have demonstrated these mechanisms and have shown that spinal injury cannot be produced simply by being exposed to a motor vehicle collision. The lack of spinal injuries as a result of rear impacts is due to the lack of the specific mechanism to produce such injuries.
This study has limitations with respect to the conclusions that can be drawn. The volunteer dataset is limited to the information provided within the published work. The pre-impact screening of volunteers was not always addressed and when it was, there was only a brief discussion. Therefore, the health of the volunteers before the testing is not known at all, or to a limited extent for most of the volunteers.
The results of this study demonstrate that the incidence of symptoms of neck pain is directly related to the change in velocity experienced by the vehicle. This trend was similar for staged volunteer testing and real-world motor vehicle collisions. The number of volunteers and exposures within the volunteer testing is sufficient to provide a high degree of certainty that injury is not expected at the delta-V levels studied, even though subjective pain may occur for a short duration. This is not a surprising outcome given the lack of reported injuries, the minor nature of the motion and forces measured during these studies, and the ongoing use of research volunteers around the world. The similarities between real-world outcomes and staged collisions demonstrate that any preparation by the volunteers does not influence the risk of neck pain. Statistical analyses of real-world rear impacts confirm the low risk of more severe injuries at impacts of similar severity to the volunteer research.